
The role of the Wheelchair Seating Therapist goes a long way further than merely helping to choose a mobility base and seat. The vision of the therapist is to give the wheelchair user and their carers the best opportunity to integrate and participate in everyday activities in the community (independence, work, learning, socialising etc.). Many studies relating to biomechanics of the human body and posture emphasis how the way we sit may affect many aspects of our lives. The Mobility Base and Seating are tools used to help achieve the ultimate care and efficiency results for the user.

While the Wheelchair User is central to all operations, experience from others also have an impact on the success of the result. The Wheelchair Seating Therapist will often see the user many times over the course of their lives and with their experience in biomechanics and products, have extensive knowledge and will ultimately make the decisions during the selection process. The Caregiver is important as they have an intimate knowledge of the user and their needs. The Technician is the installer and understands the durability required and how intuitive products are to use. The Funder or government agencies often see products after they have been used and will know well, the products which endure, are easily refurbished and recycled.
1. At your first wheelchair seating appointment the Wheelchair Seating Therapist will endeavour to gather information regarding your lifestyle, health, medical history, and independence. This helps the therapist choose the best pathway forward, enabling you to reach your greatest potential. During this session, an assessment may be carried out of your ligaments, muscles and limbs to identify their range of movement so you sit can safely sit better for longer periods. This “biomechanical” assessment is often carried out on a plinth or firm surface. Next, your body measurements are taken while you are seated in best position possible so that the best fitting wheelchair and seating is provided.
2. Your next appointment may be made once the therapist has carefully selected some options of wheelchairs and seating to trial. You may trial the wheelchairs and seating components to experience the look, feel and usability of them. Consider the environments where you might take the wheelchair and how it will be transported.
3. Once the most suitable items are selected, the therapist will write an equipment request report to acquire funding from a funding agency (government body or other). Sometimes, this process can take months before the request has been accepted.
4. On acceptance of the funding, the therapist can proceed to order the equipment, and a fitting session can be held. At this appointment, a technician will adjust every aspect of the wheelchair and seating to preset it in the optimum set-up for you. They will then go through the how to use the equipment safely. Then you can enjoy your new wheelchair & seating.
A full biomechanical seating assessment methodically encompasses many aspects about the client to ensure the best mobility wheelchair and seat is chosen and set up in the best way for the user, so their maximum potential is reached.
This is where information is gathered in depth about the client’s history, condition, previous surgery, previous mobility and seating experiences etc.
The Supine Lying assessment is carried out on a firm surface such as a plinth. The therapist assesses and records information about the user to determine symmetry and alignment, the flexibility of muscles and joints and where to correct or accommodate the posture.
The Therapist then assesses the sitting ability, balance, stability, symmetry, head control and the position of the limbs of the user in the seated position.
From the information gathered in the lying and sitting assessments the new desired posture is simulated on a firm surface or assessment chair. Once this is achieved the user is gently and slowly rocked forwards and back to find the angle of the best centre of gravity for the user (the angle of the user’s back in relation to the floor). When the Centre of Gravity is found often the user will relax their arms and find it easier to lift their head. The angle is then recorded so it can be duplicated in the new seat.
Full body measurements are taken of the user whilst seated in the new simulated posture. Each side is measured individually.

When fitting the client into a new wheelchair seat, the procedure is broken down into well-ordered sequential steps to ensure a successful result.
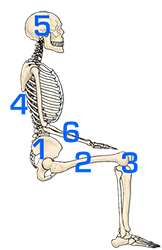
The pelvis is the largest and heaviest bone in the body. In seating the pelvis is the ‘cornerstone’. Always position and stabilise the pelvis first before attempting any other part of the seating.
Take account of hip dislocation and subluxation, relieve tightened hamstrings by lowering the knee into the contours of the cushion, take account of wind-sweeping, internal or external femoral rotation as this directly affects the position of the pelvis. Failing to accommodate wind-sweeping can increase rotation and asymmetrical shaping in the torso region.
Work downwards positioning the knees and feet as this helps to stabilise the pelvis in the seat.
Once the pelvis is stabilised in the seat the torso is a lot easier to position. An upright backrest (95 – 100°) can help with spinal extension even with users who have low postural tone. Match the backrest to the user. Locating and accommodating even small asymmetries in the user’s spine & rib cage helps to minimise spinal rotation and the development of a compensatory posture forming. Gentle support under a kyphosis or in a lordosis cavity taking care not to overbuild can increase comfort and sitting tolerance.
The position of the head is critical as in seating the head through gravity leads the body. The Headrest position set up is unique to every user and may differ depending on the support requirements, the sitting ability of the user, whether it is used for function such as head-controlled driving or merely as protection during transportation in a motor vehicle.
For users presenting with low tone and less ability to maintain their head position, it sometimes helps to provide more deeper lateral support, as restricting the lateral migration of the head often reduces the ability of the head to fall forwards.
The position of the arms helps to support the torso and can affect the Centre of Gravity of the user. Upper arms should be relaxed and in line with the torso. When the forearms are too far forward on the armrests the shoulders become protracted, and the user’s back will follow. If the forearms are too far back on the armrest shoulders may become retracted. Armrests positioned too high can cause shoulder painful elevation and armrests which are too low reduces head control and may increase the risk of a kyphosis reducing spinal extension.
Our posture, the way we hold ourselves, affects our overall wellbeing in many ways including the physiological function of our bodies, pain, pressure, stability and balance, vision, coordination and fine motor skills etc.
Posture may deteriorate with age, muscle weakness, muscle imbalance, inactivity, blocked or confused signals being sent from our brain to muscle groups and the development of compensatory postures.
When sitting in the optimum position, postural efficiency and sitting ability increases. As postural efficiency increases our subconscious effort on balance, stability and pain management reduces therefore much greater focus is able to be directed to the task at hand. This greatly increases the opportunity for improved coordination, fine motor skills and head control.
As our ability to control our own posture reduces, we must increase our reliance on external supports.

The pelvis is the cornerstone of positioning in a seat. If there is any issue with any part of a seat setup, it is important to first check the pelvis is properly positioned, as every other part of the body relies on this. The lower limb position (hips, legs, knees and feet) influences the position of the pelvis, and they can be used effectively, if positioned well, to support and stabilize the pelvis. Seat tilt and backrest angle also have a direct influence over pelvic migration and must be set at angles which the user can tolerate and encourages activity, but which doesn’t encourage slippage into Posterior Pelvic Tilt. Allowing Posterior Pelvic Tilt reduces the ability of maintaining spinal extension, reduces head control and can develop into a kyphosis over time. Also, users with Posterior Pelvic Tilt may be at increased risk of pressure injury to the Coccyx and Ischial Tuberosity regions. Another risk of Posterior Pelvic Tilt is the internal organ cavity may become restricted effecting the function of internal organs including respiration, circulation and digestion etc.
Gravity is a powerful force on an unsupported body which over time, works to form a destructive posture. Body mass and lack of movement are targets for gravity. What begins as a muscle imbalance through asymmetry can end with a change in shape of individual bones and the whole skeletal structure making a reversal almost impossible.
Postural tone relates to the continuous partial contraction of muscles. When postural tone is normal, both the flexor (closing) muscles and extensor (opening) muscles have a constant balanced tone when at rest helping us to maintain a normal posture. Abnormal postural tone occurs when muscles or muscle groups become unbalanced. This may present itself in various forms including, poor coordination and integration, abnormal sensation, jerking movements, contractures, slumped or tense postures etc.
A client with an overall LOW TONE has a floppy or limp presentation and it is often difficult to maintain spinal extension and head control.
Clients with an overall HIGH TONE present with a rigid posture. Clients with HIGH TONE are at risk of their tone increasing if they feel unstable or uncomfortable in their seating.
Many pressure issues may be traced back to bad posture. Unequal weight distribution localises and intensifies pressure increasing the likelihood of pain and a pressure sore forming.
In sitting, the position where the least intra-discal pressure on the spine, the position least affected by gravity, requires the least effort to maintain and ensures better internal organ function is an upright, straight, symmetrical sitting position. Although the optimum sitting position is determined on an individual basis through the comprehensive seating assessment the principles remain the same. Where possible:
1. The position least affected by gravity.
2. Maintain symmetry and body alignment.
3. Neutral pelvic tilt (or slightly anterior tilt), pelvis level laterally, no pelvic rotation.
4. Upright back angle 95 -100°
5. Knees & feet at 90°.
6. Femurs slightly abducted, no femur rotation
7. Upper limbs in line with torso
8. Shoulders relaxed
In circumstances where it isn’t possible to achieve the optimal sitting posture, skill is required to determine where to correct or accommodate the posture in the seat.
During our seating assessments of many “high needs” users we found that EXTENSION THRUST can apply both to clients with overall High tone or Low tone but mostly was caused by only two reasons:
1. Discomfort – Most importantly and commonly we found that tightened hamstrings combined with seating which incorporated a traditional style high pre-ischial shelf was the cause of great discomfort to the user. It seemed counter-intuitive, but enabling the leg or legs to be positioned lower to relieve the hamstring muscles combined with allowing the feet to move back on the footplate or using 90-degree leg rest hangers, the clients sat for much longer periods without extending out of the seat or showing signs of discomfort. Sometimes repositioning the legs laterally to accommodate tightened abductor muscles or adductor muscles e.g. windswept postures, greatly aided in the comfort to the user for long-term sitting. Undiscovered hip subluxation or dislocation also causes a lot of pain and discomfort to the user and the client often will extend or twist in their seating to relieve the pain. Reducing any pressure in this area and reducing the tension on the hip belt can quickly help the client to relax.
2. Mood – We all have bad days where we want to vent our feelings and frustrations. As these feelings go well beyond how they feel about their seat, this type of extension thrust will not be fixed by well configured and comfortable seating although good postural seating may reduce the frustrations making the client happier overall.

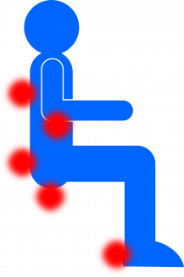
Pressure injuries are the result of prolonged pressure on the skin causing injury to the skin and underlying tissue.
Any long-term sitter (both in and out of a wheelchair) is susceptible to pressure injuries. Pressure injuries affect between 25% – 66% of all Spinal Cord Injury patients alone (excluding aged-care and medical conditions).
The risks of developing a pressure injury increase if:
1. From external pressure against the skin (such as cushions or supports).
2. From uncontrolled muscle spasms pressing or rubbing against supports.
3. From moisture (sweating, body fluids or damp seating).
 IS TIME AN ENEMY?
IS TIME AN ENEMY?How does time impact pressure? Compression + time = Pressure Injury. The risk increases if there is moisture or minimal ability to move.
Long-term sitters are most at risk!
1. Category or Stage 1. – Redness or colour change developing over bony prominence.
2. Category or Stage 2. – Shallow open ulcer or blister formed (excluding dermatitis & abrasion).
3. Category or Stage 3. – Full thickness skin loss, fat exposed.
4. Category or Stage 4. – Full thickness tissue loss with bone or tendons exposed.
Pressure redistribution is more in the domain of mechanical engineering and physics sciences rather than medical, but the results of research have far reached benefits for patients who are bedridden or wheelchair dependent.
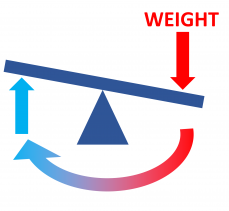
In simple mechanical terms fluid and Air Cushions work as if there were hundreds of mini seesaws operating inside the cushion. When you press down in one spot, fluid or air must pop up in another thus equalizing the overall load over the surface of the cushion.
Pascal’s Law is one of the fundamental principles of hydraulics. Blaise Pascal discovered that the pressure applied to any part of an enclosed liquid will be transmitted equally in all directions through the liquid.
Air cushions work similarly but use gas (air) in place of liquid. It is critical that both Air and Fluid cushions are only partially filled, because when pressure or weight is applied, the air and Gel filling need space to move to effectively disperse the weight.
Effective gel fluid or Air cushions transfer most of the weight vertically to disperse the pressure while limiting the horizontal spread of the cushion. Horizontal spread of the gel or air packs underweight reduces the depth of pressure redistribution.
Fluid and Air cushions are actively working and constantly changing shape to equalize pressure throughout the base.
No! There are many reasons for the development of a pressure injury, it may come down to the type of clothing, or the way we sleep. When a pressure injury develops a close look at every aspect can often find more than one reason which needs to be remedied.
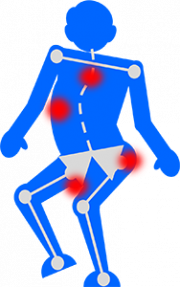
People can experience pain while using a wheelchair for various reasons including:
1. Pressure Sores: Sitting in one position for an extended period can lead to pressure sores or pressure ulcers. These occur when prolonged pressure on certain areas of the body, such as the buttocks or back, restricts blood flow and causes tissue damage.
2. Poor Posture and Alignment: Improper positioning or inadequate support in a wheelchair can result in poor posture and alignment, leading to muscle imbalances and discomfort. It can cause pain in the back, neck, shoulders, or hips.
3. Repetitive Strain Injuries: Repetitive movements, such as propelling the wheelchair using the arms, can lead to overuse injuries, such as tendonitis or carpal tunnel syndrome.
4. Musculoskeletal Issues: People who rely on a wheelchair may experience musculoskeletal issues due to reduced mobility and activity levels. Lack of regular movement and weight-bearing can lead to muscle weakness, joint stiffness, and decreased flexibility, which can contribute to pain and discomfort.
4. Spasticity: Some individuals with certain medical conditions or disabilities may experience spasticity, which is characterized by involuntary muscle contractions. Spasticity can cause muscle tightness, stiffness, and pain.
5. Equipment-related factors: Poorly fitting or improperly adjusted wheelchairs can contribute to pain. Issues such as an uncomfortable seat, inadequate cushioning, or improper positioning supports can lead to discomfort.
6. Degeneration of Musco skeletal structure: Medical conditions which cause the degeneration of the muscles or bones can cause increasing discomfort in a wheelchair. With these conditions it is important to review the wheelchair and seating often to ensure they are providing the optimal support and comfort to the occupant.
7. Internal organ pain: Prolonged sitting can cause issues to the digestive system, breathing and other organ functions. To relieve organ pain, it is important to have time out of the wheelchair and preferably in the standing position.
8. Poor circulation: After sitting for extended periods compression on arteries (such as in the thighs from the cushion or forearms from armrests) can reduce blood flow to nerves resulting in pain or numbness. Review the cushion and seat set up to ensure weight is redistributed as evenly as possible over the cushion and increase time in a position that relieves the weight from regions of compression, such as using the tilt function of the wheelchair to transfer weight from the seat to the back.
Maintain an active lifestyle to the extent possible. Engage in activities that promote movement and blood circulation, such as regular transfers, wheelchair propulsion, or participating in adapted sports.
It’s essential to address any pain or discomfort experienced while using a wheelchair as soon as possible. A healthcare professional or occupational therapist can help evaluate the cause of the pain and recommend appropriate interventions, such as adjusting the wheelchair, using proper cushioning, or engaging in physical therapy exercises.
Professional runners training for race will use a coach to analyse every aspect with the intention of gaining even a small advantage over their competitors.
With wheelchair seating, even minute alterations to the configuration can have a massive impact positively for the user.
Stabilizing the user in an efficient position, can enable the user to focus much greater effective effort towards the task at hand. Fine motor skills improve when sitting ability improves.

